What is Chronic Obstructive Pulmonary Disease (COPD)?
Chronic Obstructive Pulmonary Disease (COPD) is a progressive lung disorder characterized by persistent airflow limitation. It mainly includes chronic bronchitis (chronic cough for at least three consecutive months in two consecutive years) and emphysema (destruction of alveoli). The leading cause is long-term exposure to irritants such as cigarette smoke, biomass fuel, and air pollution.
Pathophysiology
COPD develops due to chronic inflammation in the airways and lung parenchyma:
- Airway inflammation: Exposure to irritants activates macrophages, neutrophils, and CD8+ T-cells.
- Mucus hyper secretion: Goblet cell hyperplasia leads to excessive mucus → airway obstruction.
- Ciliary dysfunction: Impaired clearance of mucus and pathogens.
- Alveolar destruction (emphysema): Loss of elastic recoil → air trapping and hyperinflation.
- Small airway narrowing: Fibrosis and inflammation reduce airflow.
- Gas exchange impairment: Leads to hypoxemia and, in advanced cases, hypercapnia.
Signs and Symptoms of COPD
The patients may present with the following signs and symptoms.
- Chronic cough (often productive)
- Dyspnea (progressive, worse on exertion)
- Wheezing
- Chest tightness
- Prolonged expiration
- Use of accessory muscles
- Barrel-shaped chest (hyperinflation)
- Cyanosis (late stage)
- Peripheral edema (cor pulmonale)
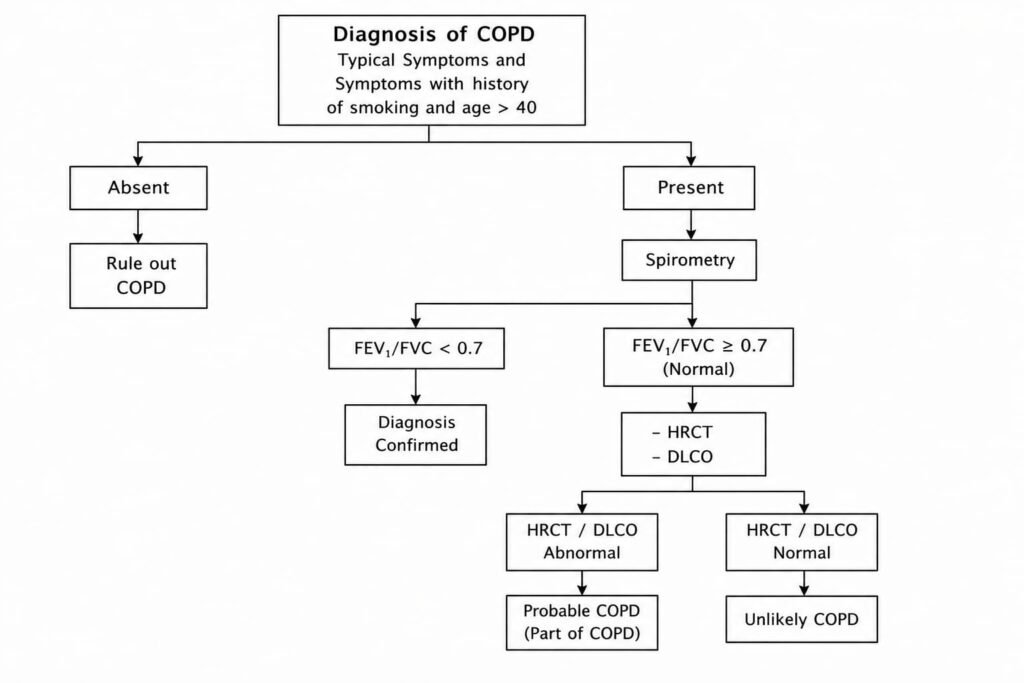
Diagnosis of COPD
Clinical Evaluation
- History of smoking or exposure to pollutants
- Persistent respiratory symptoms
Investigations
- Spirometer (gold standard): FEV₁/FVC < 0.7 confirms airflow limitation
- Chest X-ray: hyperinflation, flattened diaphragm
- ABGs: assess oxygenation and CO₂ retention
- Pulse oximetry: SpO2 Level
- CT scan (if needed for complications)
Management of COPD
Management of COPD aims at slow down the disease progression and reduce symptoms. The treatment ranges from non-pharmacological measures to pharmacological therapy.
1. Non-Pharmacological
- Smoking cessation (most important step)
- Pulmonary rehabilitation
- Vaccinations (influenza, pneumococcal)
- Long-term oxygen therapy (in severe hypoxemia)
2. Pharmacological
- Bronchodilators:
- Short-acting (SABA, SAMA) for relief
- Long-acting (LABA, LAMA) for maintenance.
- Oral bronchodilators: theophylline is recommended only when other treatment options are not effective enough. These are used with quite precautions.
- Inhaled corticosteroids (ICS): for frequent exacerbations
- Combination therapy: LABA + ICS or LABA + LAMA are preferred as maintenance treatment.
- Phosphodiesterase-4 inhibitors: Roflumilast is recommended in severe cases.
- Antibiotics: during exacerbations if infection suspected. Azithromycin 500mg thrice a week reduce exacerbation but QTc, Lfts and hearing should be monitored.
3. Advanced Interventions
- Non-invasive ventilation (NIV)
- Surgical options (bullectomy, lung volume reduction, transplantation in selected cases)
Complications of COPD
- COPD exacerbation, where symptoms suddenly worsen due to infection or pollution.
- Recurrent lung infections like pneumonia.
- Respiratory failure with low oxygen and high carbon dioxide levels.
- Pulmonary hypertension leading to strain on the heart.
- Right-sided heart failure (cor pulmonale) and reduced quality of life.
Compliance (Adherence to Treatment)
Patient compliance is critical in COPD management:
- Education: Understanding disease progression and inhaler use
- Correct inhaler technique: Ensures drug effectiveness
- Regular follow-up: Monitor symptoms and lung function
- Lifestyle modification: Avoid triggers, maintain physical activity
- Medication adherence: Skipping doses worsens outcomes
- Psychological support: Anxiety and depression can reduce compliance
Conclusion
COPD is a chronic, preventable, and manageable disease. Early diagnosis, smoking cessation, appropriate pharmacotherapy, and strong patient compliance significantly improve quality of life and reduce disease progression.